Coastlines 写了: ↑06 9月 2025, 15:29我不敢做器官donor,我怕疼
我佩服敬佩做器官donor的
我也怕火化,不敢想,我觉得太残忍了,但人死了怎么处理都不好,算了,别想了
 我佩服敬佩做器官donor的
我佩服敬佩做器官donor的这个时候人都死了、
活着我也不敢,佩服那些捐肾的
版主: resso
Coastlines 写了: ↑06 9月 2025, 15:29我不敢做器官donor,我怕疼
我也怕火化,不敢想,我觉得太残忍了,但人死了怎么处理都不好,算了,别想了
这个时候人都死了、
活着我也不敢,佩服那些捐肾的
Leuning 写了: ↑06 9月 2025, 13:37Michigan donor registry drops amid national organ donation probe https://share.google/FdCxHbDSqUOXbDnmj
Read the subtitle: Gift of Life Michigan urges public to seek facts before deregistering
这种是要人死了才能采集器官的。
个例当然要调查,但是不能一杆子都打死。
摸摸头
mmt 写了: ↑06 9月 2025, 15:53Leuning 写了: ↑06 9月 2025, 13:37Michigan donor registry drops amid national organ donation probe https://share.google/FdCxHbDSqUOXbDnmj
Read the subtitle: Gift of Life Michigan urges public to seek facts before deregistering
这种是要人死了才能采集器官的。
个例当然要调查,但是不能一杆子都打死。
没有不同意,所以我只是说现象:注册的人减少,原因是负面新闻。
(小)泡子子
这绝对不是“极少数的意外”。《纽约时报》披露的仅是冰山一角。美国官方的结论是:HHS Finds Systemic Disregard for Sanctity of Life in Organ Transplant System (https://www.hhs.gov/press-room/hrsa-to- ... se%20cases.)
7月份美国卫生与公众服务部长小罗伯特·F·肯尼迪专门对此发表讲话。他说:
“Our findings show that hospitals allowed the organ procurement process to begin when patients showed signs of life, and this is horrifying,” Secretary Kennedy said. “The organ procurement organizations that coordinate access to transplants will be held accountable. The entire system must be fixed to ensure that every potential donor’s life is treated with the sanctity it deserves.”
鉴于事态严重性,美国卫生部门已经着手对器官摘取进行整顿改革。https://www.hhs.gov/press-room/hrsa-to- ... se%20cases.
我个人观点:
目前阶段,为帮医院个忙,还是不注册为好。
我不在医院系统,以下是纯粹我自己的观察,推测。
医院故意为摘器官,不抢救。这个从motivation上讲,不合常理。医院又拿不到任何经济利益。
但是,这种情况在美国各地都出。为什么呢?
我推测是医院管理问题。急诊医人进来后被编号,建档。医生不固定,下一个医生先看病人档案,再采取措施。
急诊室救人已经手忙脚乱,加个摘器官,不是更乱? 摘器官和救人从技术人背道而驰。接班的医生按档案摘器官,他/她不必负任何责任。 但如果他/她不先入为主,继续努力抢救,说不定可以救你一命。但是,从医生角度来看,这是额外工作量。
如果你没注册,那接班医生会继续抢救。这不是帮医院减少混乱吗?
(小)泡子子
我不同意 Leuning 的“医院又拿不到任何经济利益”这种说法。由于器官移植手术本身的高昂费用以及后期费用,医生、医院、制药公司都从中获利。
How doctors are compensated
Instead of profiting from the organs themselves, transplant surgeons and physicians are compensated through standard medical billing processes for their complex services.
Work Relative Value Unit (wRVU): This common model compensates doctors based on the volume and intensity of their work, such as the complexity of a surgical procedure or the amount of time spent on patient care.
Performance-based incentives: To encourage more transplants and better outcomes, the Centers for Medicare & Medicaid Services (CMS) have tested models that financially reward hospitals and doctors based on performance metrics.
Financial benefits for the medical system
The entire medical system financially benefits from the organ transplantation process, which involves extensive care and resources.
Hospitals and transplant centers receive substantial payments from insurance companies and government programs like Medicare for the complex surgeries and extensive pre- and post-transplant care. For some hospitals, a successful transplant can be a very lucrative procedure.
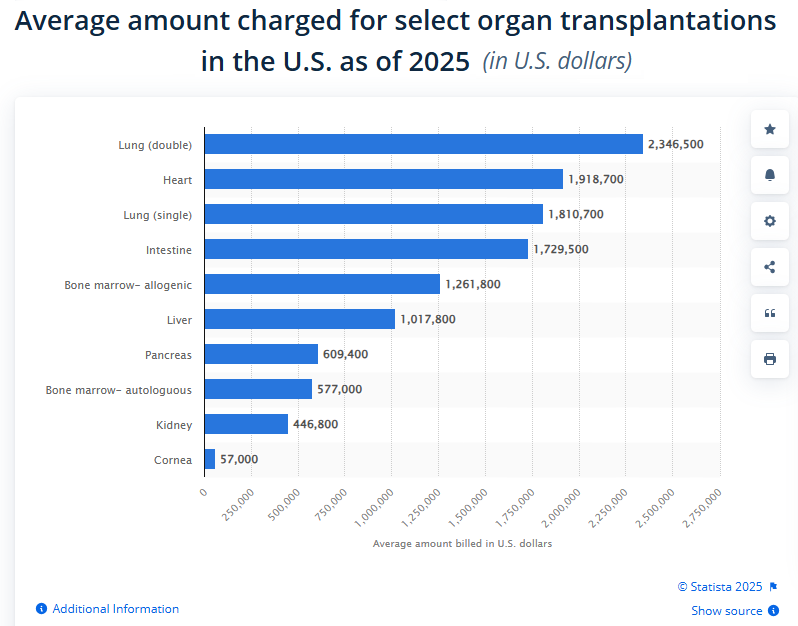
The total billed cost for a single transplant is high, ranging from hundreds of thousands to over a million dollars, depending on the organ.
Pharmaceutical companies benefit from the high cost of immunosuppressant drugs that transplant patients must take for the rest of their lives. Pharmaceutical payments to transplant doctors for consulting, travel, and speaking can also influence the field.
Leuning 写了: ↑06 9月 2025, 16:38我个人观点:
目前阶段,为帮医院个忙,还是不注册为好。
我不在医院系统,以下是纯粹我自己的观察,推测。医院故意为摘器官,不抢救。这个从motivation上讲,不合常理。医院又拿不到任何经济利益。
但是,这种情况在美国各地都出。为什么呢?
我推测是医院管理问题。急诊医人进来后被编号,建档。医生不固定,下一个医生先看病人档案,再采取措施。急诊室救人已经手忙脚乱,加个摘器官,不是更乱? 摘器官和救人从技术人背道而驰。接班的医生按档案摘器官,他/她不必负任何责任。 但如果他/她不先入为主,继续努力抢救,说不定可以救你一命。但是,从医生角度来看,这是额外工作量。
如果你没注册,那接班医生会继续抢救。这不是帮医院减少混乱吗?
现在医院系统的首要问题: 人手短缺。连正常的急救任务也完不成:
How the Covid pandemic left healthcare workers burned out and demoralized https://share.google/8nNnHcJgU9pdV51HS
(小)泡子子
shepherd17 写了: ↑06 9月 2025, 16:52我不同意 Leuning 的“医院又拿不到任何经济利益”这种说法。由于器官移植手术本身的高昂费用以及后期费用,医生、医院、制药公司都从中获利。
How doctors are compensated
Instead of profiting from the organs themselves, transplant surgeons and physicians are compensated through standard medical billing processes for their complex services.
Work Relative Value Unit (wRVU): This common model compensates doctors based on the volume and intensity of their work, such as the complexity of a surgical procedure or the amount of time spent on patient care.
Performance-based incentives: To encourage more transplants and better outcomes, the Centers for Medicare & Medicaid Services (CMS) have tested models that financially reward hospitals and doctors based on performance metrics.Financial benefits for the medical system
The entire medical system financially benefits from the organ transplantation process, which involves extensive care and resources.
Hospitals and transplant centers receive substantial payments from insurance companies and government programs like Medicare for the complex surgeries and extensive pre- and post-transplant care. For some hospitals, a successful transplant can be a very lucrative procedure.
The total billed cost for a single transplant is high, ranging from hundreds of thousands to over a million dollars, depending on the organ.
Pharmaceutical companies benefit from the high cost of immunosuppressant drugs that transplant patients must take for the rest of their lives. Pharmaceutical payments to transplant doctors for consulting, travel, and speaking can also influence the field.
Leuning 写了: ↑06 9月 2025, 16:38我个人观点:
目前阶段,为帮医院个忙,还是不注册为好。
我不在医院系统,以下是纯粹我自己的观察,推测。医院故意为摘器官,不抢救。这个从motivation上讲,不合常理。医院又拿不到任何经济利益。
但是,这种情况在美国各地都出。为什么呢?
我推测是医院管理问题。急诊医人进来后被编号,建档。医生不固定,下一个医生先看病人档案,再采取措施。急诊室救人已经手忙脚乱,加个摘器官,不是更乱? 摘器官和救人从技术人背道而驰。接班的医生按档案摘器官,他/她不必负任何责任。 但如果他/她不先入为主,继续努力抢救,说不定可以救你一命。但是,从医生角度来看,这是额外工作量。
如果你没注册,那接班医生会继续抢救。这不是帮医院减少混乱吗?
医院赚钱好像Based on medical code. 因为我没这方面专业知识,所以不敢下判断说医生有动机。
(小)泡子子
